
Swimming in a (Fluoridated) Sea of Inadequate Data
On the history of fluoride and the new NTP Fluoride and IQ Meta-analysis

A new meta-analysis published in the JAMA Pediatrics suggesting that fluoride is harmful for children’s IQ is making waves. This post takes a longer look at the history of water fluoridation for dental health, the long-time opposition to fluoridation, the evolving but weak evidence on fluoride’s potential hazards, and the failure of the USA research establishment to seriously fund research on environmental exposures throughout key developmental periods.

I did my PhD in Nutrition at Cornell in the city of Ithaca and got my first and only cavity within a few years of living there. While I considered the cavity may have resulted from changing dietary habits (hello, gradschool stress-relieving sugar excursions), I also learned that Ithaca’ water was not fluoridated. I decided to look into the history of water fluoridation in Ithaca and discovered that Clive McCay, a famous nutrition researcher at Cornell (who is credited as one of the first showing that caloric restriction impacts lifespan in rodents) was an OG fluoride skeptic of sorts in the 1950s and 60s when national debates about water fluoridation were ongoing - he expressed concern on a radio program in Ithaca that he was not convinced of fluoride’s benefits to teeth and was worried that there were long-term effects on the thyroid and kidney. Decades later, Ithaca still didn’t have fluoride in the water and I had my first cavity. Thanks, Clive.
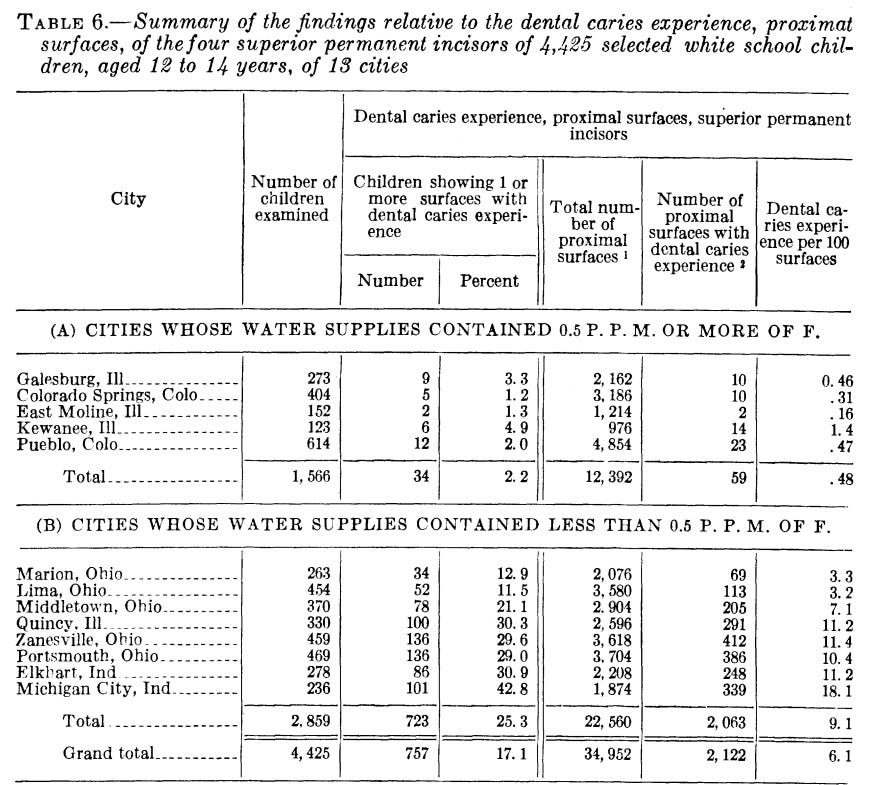
The history of fluoride begins with another McKay (though with a K, not C) - Fred McKay was an early 20th century dentist in Colorado Springs who noted that there were brown stains on many of his patients teeth (mottled teeth, now referred to as dental fluorosis) and he suspected it was from something in the water. Others across the globe would report a similar “Rocky Moutain Mottled Teeth” phenotype. McKay would ultimately gather together samples from communities with a high degree of tooth mottling and found that all were high in naturally occurring fluoride , confirming findings in rodents (1931) that was able to reproduce a mottled enamel with added sodium fluoride . The mottling was initially seen as a problem and researchers sought to find alternative water sources and ways to remove fluoride from the water; however, in the course of investigating the cause of the mottling, a dentist and researcher in the UK named Norman Ainsworth would note that in areas where teeth were mottled, they also had less dental decay - providing the first indirect hint that fluoride exposure might be protective against tooth decay. These observations would ultimately lead to a famous ecological investigation called the “21-City Study” conducted by HT Dean, a dentist appointed by the US Public Health Service - the 21 City Study was conducted in 4 states (indiana, Illinois, Ohio and Colorado) across 21 cities where the fluoride and other mineral contents of the water naturally varied. The data from this study was some of the first to indicate that protective effects of fluoride could occur at levels that resulted in minimal mottling (note: this evidence is considered relatively weak ecological data by modern standards)
These early observations would launch a broader effort by health authorities to pilot artificial water fluoridation (i.e. bringing areas with naturally low levels of fluoride up to levels ~1 ppm or 1g/L). Foundational trials in 4 cities receiving fluoridation (vs 4 neighboring ‘control’ cities) were initially selected for a 15 year trial, and 2 additional cities with natural fluoride ~1ppm were also selected to compare artificial vs natural fluoridation to. In 1945, Grand Rapids Michigan would become the first city in the world to artificially fluoridate its water supply (its neighbor city, Muskegon, was its control). By the late 1940s and early 1950s, results from the foundational trials showing lower numbers of cavities in children would roll in, including the Grand Rapids-Muskegon comparisons; the planned 15 yr comparison wouldn’t ultimately happen when Muskegon opted to withdraw from the trial and fluoridate its water. Other trials were also undertaken outside the USA, including ones in Canada, the Netherland, New Zealand, the UK and Ireland, all reporting reductions in tooth decay in artificially fluoridated areas and no major change in control towns. In 1950, The American Dental Association and US Public Health Service endorsed water fluoridation and a large number of cities would adopt this practice (by 1969, 43.7% of Americans were estimated to have access to fluoridated tap water). Optimal fluoride levels for dental health were initally set in the range of 0.7ppm to 1.2ppm, though notably, at this time, fluoridated dental products weren’t quite mainstream, so these levels were established with the idea that water fluoridation was the major source of fluoride alongside the smaller amounts that naturally occurs in foods (Crest technically released the first fluoridated toothpaste in 1956 but these wouldn’t become quite mainstream until the mid 1960s-1970s).
The history of community-level water fluoridation is typically considered a public health success - relatively clear health benefits for dentition were established through quasi-experimental studies and water fluoridation was rapidly taken up (note again: this data is not considered as high quality from modern perspectives; large, randomized cluster trials randomizing many communities to fluoridated water and modeling the data with more advanced statistical methods would be ideal). The success of water fluoridation didn’t occur without some opposition, well beyond Clive McCay’s modest concerns noted above. By 1957, Donald McNeil had written “The Fight for Fluoridation”, detailing the history of fluoride in the USDA and its various opponents, including layfolk, chiropractors, and religious figures. The reasons for opposition for varied, including libertarian style thinking about freedom of choice to consume unfluoridated water, to health concerns with some thinking fluoride is a poison being added to water, with the latter having a subgroup of activists who perceied water fluoridation as a communist plot to take over the country (truly, history loves to repeat itself). Gretchen Ann Reilly wrote an excellent chapter on this titled “Not A So-Called Democracy” in the “The Politics of Healing: Histories of Alternative Medicine in Twentieth Century North America”.

Fluoridation has continued to be a contentious topic, with virtually any and all ails that can affect the human body being ascribed to fluoride since its addition to the water supply. Complaints of fluoride causing teeth to fall out were reported to health officials in Grand Rapids, before the fluoride was actually added to the water. Strident (also phantom) claims around fluoride have existed well into recent history, with a community (Kuopio) in Finland in 1992 complaining of symptoms from water fluoridation during a period that the water fluoridation had unknowing been stopped - a great examples of how the human psyche can influence the perception of health effects and how readily we can be primed to find associations that aren’t causal.


Not all of the concerns about fluoride, however, are total crackpot theories.
Before we dive into thinking about safety, let’s lay some ground work. Flouride is the ionic (F-) form of the element, fluorine, and its present nearly ubiquitously (soil, water, plants, animals)- i.e. it is something that is virtually impossible to not be exposed to. In debates about fluoride’s health effects, I’ve witnessed a general feeling of “I don’t want this in my body” in response to discussions of artificial water fluoridation, but it’s not really possible to not be exposed to fluoride because its everywhere - the scientific discussion is about how much you’re exposed to and through what sources. While there is concern about the ‘artificial’ nature of water fluoridation, it’s important to note that levels of naturally occuring fluoride in the water vary and you can readily find mineral waters with higher levels than artificially fluoridated water (the EU sets a max of 5mg/L and there must be labeling for mineral waters sold with >1.5mg/L) - as we’ll get to below, the signal for health concerns in human studies comes almost entirely from studies comparing naturally high vs low fluoride levels, not from community water fluoridation. The ubiqutiy of fluoride in the environment actually contributed to research in rodent experiments that indicated impaired growth with low levels of flouride diets and resulted in its consideration as an essential nutrient in 1974; however, while flouride is found naturally within the body from our exposure to it in the environment and accumulates in the skeleton, it is currently not considered essential for life ( there is no known essential physiological process which it supports and the evidence for its requirement for normal growth is not reproducibly seen in animal models).
In general, we think of fluoride as a ubiquitous exposure with potential health benefits (i.e. reduced tooth decay/cavities), but not required for life. This model is important, because for exposures without health benefits, we typically take a purely toxicological approach to its regulation: identifying the lowest levels associated with detrimental effects (LOAEL - lowest observable adverse effect level) and the level associated with no detrimental effect (NOAEL), divide the NOAEL by a safety factor (commonly 10-1000x), and set this as an upper limit of exposure to ensure a low likelihood of acute or chronic toxicity. However, given fluoride’s ubiquitous exposure and potential benefit, there is a need to identify a broad dose-response relationship to ensure levels of exposure are both safe and effective; it is expected that fluoride can be hazardous (i.e. there will be some level of exposure where harm is observed) but the goal is to assess risk (i.e. the concentration of fluoride exposure where that harm occurs) - we’ve long known that negative effects can occur from fluoride exposure because this all started with enamel mottling. The goal is to make sure that total exposure from dental products and water fluoridation (natural or artificial) provides the maximum benefit that can be provided while not negatively impacting any other health outcome.
When it comes to toxic effects of fluoride (or any compound for that matter), we typically think about acute toxicological outcomes (e.g. vomiting, respiratory or cardiac problems, death), chronic exposure outcomes (eg developing cancer) as well as reproductive and developmental outcomes (e.g. does exposure influence the ability to get pregnant or carry pregnancies to term; does it alter the development of organ systems and their functions). There is a reasonable literature base that has investigated fluoride exposure in relation to a number of acute, chronic, reproductive and developmental outcomes in rodents and identified NOAEL and LOAELs with varying but reasonable degree of confidence for specific outcomes; fortunately, the data largely demonstrates that total human fluoride exposures - not just from fluoridated water but food and dental products - at the high end of exposures (between 50-120ug fluoride/kg body weight per day) are still well below the NOAEL and leave a margin of error ~20-50 fold (i.e. humans with very high exposures from highly fluoridated water ~4mg/L still do not reach the doses on a per kilogram basis that still caused no effects in mice). Much of this toxicological evidence was reviewed by the National Acadmies of Sciences in 2006 when reviewing the EPA’s maximum contaminant levels for fluoride in water (ie not determining the beneficial amount but the maximum amount where there is not apparent risk). The committee would ultimately recommend to reduce the maximum contaminant level goal for flouride to less than its current standard at the time of 4mg/L - there wasn’t consistent convincing evidence for concern for any health outcome apart from the risk of dental flourosis (mottling) from children with high exposures. The impetus for this report was not entirely artificial fluoridation levels (where levels are raised to 0.7-1.2mg/L) - it was primarily driven by concerns for vulnerable subpopulations including over a million people in the USA with natural fluoride concentrations between 2-4+mg/L that are also receiving exposure from use of fluoridated products. The committee was ultimately concerned that some children were at risk for enamel mottling (and potentially brittle bones more at risk of fracture from high life long exposure) with maximims of 4 mg/L and thus, recommended lowering this level.
The National Academies committee reviewed the literature on many other health outcomes at the time, using both animal models of exposure to fluoride as well as epidemiological associations of fluoride exposure and child health outcomes - these human studies are non-experimental/non-randomized, and in medicine we typically think of them as much lower quality, but given the ethical issues in randomizing individuals to fluoride to look for negative health outcomes, the risk assessment relies heavily on these imperfect lines of evidence. The committee found, for example, little concern for reproductive effects due to adverse effects only occurring at very high exposure levels unlikely to be encountere by anyone in the USA. It noted, however, that emerging data out of China, where children regularly exposed to naturally highly fluoridated drinking water (2.5-4+mg/L), reporting IQ deficits, though the quality of these studies were limited. Animal studies available to the committee at the time were limited, frequently used high doses (>10mg/L) and found changes in anatomical and molecular features in the brain but only small effects on behaviors - the committee noted the need for study relevant concentrations on a wide range of cognitive domains and better understand mechanisms. The results of this 2006 report are frequently cited by activist groups like the Fluoride Action Network as evidence of concern for fluoride and IQ and were cited in the National Toxicology Program (NTP)’s 2015 impetus for undertaking a broader effort to assess fluoride in relationship to health outcomes like neurocognition, cancer and endocrine disruption. Thus, we arrive at the modern controversy.