
On Infant Formula & Operation Stork Speed
A History and contextualization of infant feeding

This week we had a new announcement from HHS that the FDA will be launching “Operation Stork Speed”, an effort to take a look at infant formula in the USA. There’s a lot in here that sounds good (although scant on details) that calls for updating the nutrient composition of formula, better regulations around heavy metals, improving transparency and potentially funding better research.

At a high-level, this is much needed - we are coming off the backs of a massive infant formula shortage following the shutdown of a plant in Michigan that revealed the detrimental impacts of the extreme market consolidation in the industry. Parents are regularly met with (often-misleading) headlines about levels of heavy metals in foods for infants/children - we just had one this week about metals in infant formula despite the levels being below both USA and EU safety standards. Parents and clinicians also have to navigate an infant formula market that is replete with (rarely supported) claims made by manufacturers about their product having the optimal composition for infant health and development. Add to this mix all of the health influencers saying that infant formula is feeding your baby poison because of the toxic GMOs, seed oils, and sugar, and you’ve got the recipe for a nightmare situation where parents/caregivers are afraid to feed their kids. There is an obvious need for the government to try to improve trust and ensure a marketplace that the most basic infant formula products provide what is likely to be best for infants health & development - the only people benefiting from the distrust and fear are folks with something to sell.

Whether the current administration is up to the task of addressing the infant formula landscape remains to be seen, and the details in Operation Stork Speed are a bit scant (to be frank: I’m not confident given the current cuts at FDA but we’ll see if there’s a reversal). I figured it would be worthwhile to write a primer post that orients folks to some of the interesting history on the development of infant formula and how we landed where we are today. From there, I’ll also comment on some considerations for how we actualize having the safest and most quality infant formulas, and address sensational claims around toxic ingredients. The history also provides a nice reference point for how risky infant formula practices have been, how far we’ve come, and how relatively privileged we are to be debating about some of the topics that dominate today’s conversations.
Before we dive in, I want to note up front that breastfeeding is considered the gold-standard for infant feeding and there’s a whole lot the administration could do to promote and facilitate this but that’s beyond the scope of this post. There are innumerable reasons why a mother/caregiver may choose not to or be unable to breastfeed or feed human milk and we should prioritize supporting feeding autonomy and optimizing outcomes regardless of the feeding approach (‘fed is best’).
History
The best way to feed infants who cannot be fed breastmilk exclusively has long plagued humanity. Wet nursing might be the first thing that someone thinks of when considering alternatives to direct mother-to-infant breastfeeding and wet nursing is indeed seen throughout history and across cultures; however, it was often only available to the afluent in societies and/or was stigmatized in some cultures. Thus, infants who were unable to be breastfeed (many reasons from milk supply issues to high rates of maternal mortality, etc) had to be fed alternatives. Histories of infant feeding practices detail all sorts of unsafe modalities (even feeding beverages that contain alcohol!) that will make you long for the modern convos about the relative safety of GMO seed oils.
When looking for breast milk alternatives, it is probably unsurprising to most readers that many cultures turned to animal’s milk (the animal source depended upon the culture but references include everything from goats to camels to pigs and cows). I want to be very clear that, from a modern scientific perspective, we now know that unprocessed/unmodified animal’s milk is unsafe for infant feeding - the higher protein and mineral content (sodium, phosphorus) can cause GI bleeding, stress the underdeveloped infant kidney, and cause electrolyte abnormalities. Animal milk also typically provides inadequate amounts of a number of essential nutrients, including iron, vitamin D, vitamin C, folate and essential fatty acids. Raw animal milks are also at risk of being contaminated with pathogens and infants have relatively underdeveloped immune systems. These issues with animal milk feeding can result in serious sequelae including impaired growth and bone mineralization, lasting neural and behavioral impacts and death from metabolic and infectious etiologies. I stress this issue because we’ve reached the abjectly dangerous point in the online discourse where infant formulas are portrayed as so hyperbolically toxic that it is not uncommon to find recommendations to feed animal’s milks, often raw (goat is the most commonly recommended despite documented case studies of its harm to infants).

Our modern understanding of the risks of animals milk for infants benefits from knowledge of chemistry, physiology and human nutrient requirements. However, if you try to place yourself back in time, particularly back to the 18th-19th centuries when there was significant interest in alternative infant feeding strategies, identifying whether animal milk was suitable for infants was challenging. Milk could be life-saving if the alternative was abject starvation; it could also be a source of pathogens (pasteurization was not common until the early 1900s), harm vulnerable infants due to its native compositional issues noted above, be a source of contaminants (e.g. nitrates, plant toxins in milk), and be processed in ways that are harmful (heat-treatment destroys vitamin C and infantile scurvy was a big issue during the 19th century). Any observer could reasonably conclude animal milks were both the perfect food or harmful and you can indeed find accounts of either perspective. The harms perceived from milk nevertheless led to efforts to find alternatives.

The 19th century saw important advances in our basic understanding of the macronutrient composition of foods generally, including human and cow’s milk, that laid the foundation for efforts to modify animal milks to be suitable for infants (note: the concept of essential micronutrients were not established for the most part at this time). The first chemical composition of cow and human milk was published in 1838 by Johan Franz Simon, with much work followed by Arthur Meigs into the 1900s, that ultimately concluded human milk was higher in carbohydrate (lactose) and lower in protein than cow’s milk, with some observations that the protein was more resistant to acid hydrolysis. These findings led to efforts by a number of scientists and physicians to modify the carbohydrate and protein composition of milk through mechanisms like the addition of water and starch to milk and treatment of milk with rennet (proteolytic enzymes from cow stomach that digested the milk protein to make it easier on the infant digestive tract). While relatively unsophisticated, this notion of modifying cow’s milk to more closely match the composition of human milk underlies much of the philosophy still present today as we try to make infant formula’s match as close to breast milk as possible.
The most famous effort to modify cow’s milk was undertaken in the mid 19th century by the organic chemist and one of the pioneers in nutrition science, Justus von Liebig. Liebig had a daughter who struggled to breastfeed and he sought to create an ‘artificial’ human milk replacement - his formulation was relatively crude by modern standards, relying on 1 part wheat flour and 10 parts skimmed cow’s milk with the addition of potassium bicarbonate. Liebig’s big innovation was the inclusion of malt, flour made from grains that had started to germinate and had higher levels of amylase, capable of breaking down the starch into glucose that can be absorbed by infants (adults produce their own amylase but the infant salivary gland and pancreas produce low to no amylase in the first months of life and thus struggle to break down starch to utilize its glucose for energy). Liebig put the recipe out into the public domain and controversy erupted following reports of infants dying after being fed the formula. The Science History Institute has a good article/podcast covering this controversy. Liebig patented his formulation and spurred a huge industry a number of competitors by the end of the 19th century, essentially marking the beginning of the commercialization of infant feeding. Physicians got involved heavily in infant feeding in this era as well, with a precise method for modifying milk with water, cream and sugar popularized by Rotch.


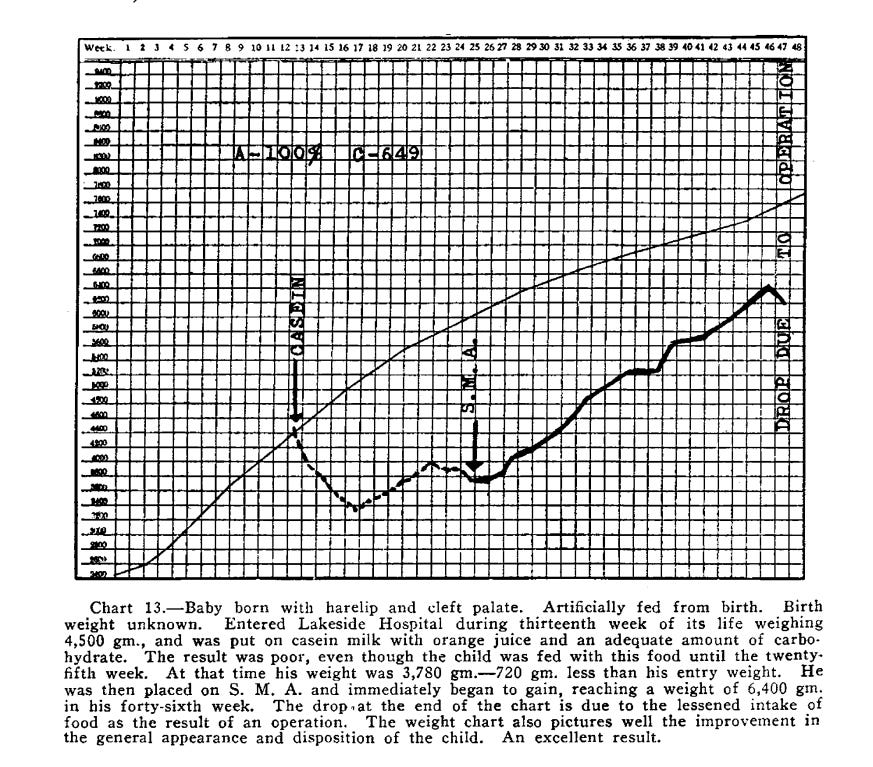
The general knowledge about human milk composition led to the basis of the modern formula emerging in 1915 - the formula was “Synthetic Milk Adapted”, developed by Gerstenberger, and contained nonfat cow milk, added lactose, oleo oils and vegetable oils. This was commercialized as “SMA” in 1919 with the addition of cod liver oil (a known remedy to prevent vitD deficiency/rickets at the time). Gerstenberger published his results of using SMA for 3 years in a number of cases of infants failing to thrive that showed a relative resumption of normal growth upon feeding. Other notable players in the formula industry space emerged at this time, including Nestle and Mead Johnson. Bosworth & Bowditch, prolific researchers in infant formula mineral and fatty acid composition, produced research that ultimately led to a formula that would be renamed ‘Similac” (the basis of the modern Similac brand owned by Abbott).

Despite early development, formulas didn’t become a huge market until the 1960s, predominantly due to the use of cheap and shelf-stable evaporated milks. Milk evaporation without added sugar emerged in the late 1800s but wasn’t initially used for infant feeding due to concerns about inducing infantile scurvy. However, in the 1920s, it became more customary to supplement the diet of infants with fruit and vegetable juices, providing an alternative source of vitamin C and facilitating the use of canned evaporated milks. Evaporated milks had the added bonus of the heat-treatment both killing pathogenic microorganisms as well as denaturing proteins and improving digestibility. In early trials, evaporated milks supported growth similar to breastfed infants, leading to physicians recommending their use widely.

By the mid-20th century, both evaporated milk-based home formulations as well as SMA-like commercial formulations were available but there was little in the way of legislation to standardize the nutrient composition of formula. Unsurprisingly, problems emerged; these included the high renal solute load of formulas (determined by the protein and electrolyte content of formulas —> increasing the risk of dehydration and electrolyte imbalances that can cause severe harm/death), low bioavailable iron content (increasing the risk of anemia that can influence the risk of cognitive and motor developmental issues, as well as infections), low vitamin C content (increasing the risk of scurvy, still relatively prevalent at the time), and low intakes of essential fatty acids. Incidences of fat (vits K, D) and water soluble (folate) vitamin inadequacies were also reported at the time. Isolated incidences of infant nutritional inadequacies can be found throughout the literature but it was ultimately 2 major incidences that catalyzed regulation of the industry.
Modern Regulation Emerges